After over 1.2 million FUE grafts taken by the Cole Isolation Technique (CIT™) and over 1000 results by FUE, I have developed many techniques and noted many aspects of this procedure that insure consistent quality results. The first thing I noted was that one must recognize that no two people are created equal. It follows that no two donor areas are equal. Therefore, it is imperative that one have a wide variety of techniques and tools in order to achieve consistent results regardless of the donor area characteristics.
In the spring of 2003 I first introduced the 0.75 mm punch to FUE. I introduced this smaller punch for the simple reason that I postulated that smaller incisions might produce a better aesthetic donor region. I immediately noted that I it had certain advantages and certain disadvantages. The advantages included a smaller surface incision and easy removal of smaller follicular units or groups. The disadvantages included greater adverse risks to hair follicles in many instances. These risks included damage to the follicular sheath, transaction of the hair shafts, a lower number of hairs per follicular unit, generally a less consistent result, and inability to manage some donor regions at all.
To our surprise it was apparent that incision sites were smaller with the smaller punch, but the end result was the same regardless of punch size. In other words, the donor area healed equally well or the same regardless of the punch size. The rationale for this is quite simple. FUE is generally a shallow incision unlike a strip surgery. In order to understand this, you must recognize that FUE involves the removal of minute isolated regions of dermis, epidermis, and adipose that amount to tiny increments in terms of cubic millimeters. This is the opposite of a strip procedure where it is not uncommon to remove 20,000 or over 30,000 cubic millimeters of contiguous tissue in a single procedure. CIT™ involves removal of isolated areas of about 2 cubic millimeters. There are some basic tenets in cosmetic surgery. One of the most important with regard to skin surgery is that tiny incisions heal without visible scars to the naked eye. In other words, once you exceed certain limits scarring is apparent, but below these limits scarring is a non-factor.
It stood to reason to me that there simply was no rational long term reason to micro-manage all donor areas provided that the risks exceeded the rewards. I remain resolute in this conviction especially in the light that I have seen numerous clinics and physicians follow my lead with the 0.75 mm punch and even smaller punch sizes over the past 4 years yet they have put up comparably a minimal number of quality results. The reason for their obvious lack of parallel numbers of quality results is quite simple when you consider the risk/reward ratio involved with exclusive use of smaller punches. It is true that when you utilize smaller punches, you will have some quality results, but overall you will not be consistent. When the only tool you have in you belt is a hammer, every patient must be a nail. Once again, every patient is slightly different. Therefore, one must have a full array of tools in order to affect a consistent, quality outcome.
As stated in my vast experience with this procedure, I noted that no single method or instrument worked equally well on all individuals. I found quickly that no one technique or procedure worked equally well for ever patient. This is because every donor area is different and one had to be able to adapt to these differences. For this reason, I began developing a number of different devices of a variety of geometric shapes. All of this development was quite costly. Therefore, we were quite careful about our disclosures and we also sought patent protection on a number of the instruments. From the early days we planned to offer our procedure and instruments through a license so that we can continue developing better tools and instruments that we hoped would encourage more physicians to abandon the invasive, unpredictable scar prone strip procedure. That time is here.
Over the past years, we have heard many new physicians and clinics promote smaller punch sizes exclusively because they produce less scarring. Over the years we have listened to this rhetoric with concern because we know from greater experience that one must be able to adapt to the differences in the donor area if you are going to produce consistent results. Some clinics have now been promoting such instrumentation for over 4 years yet they continue to produce inconsistent results.
Anecdotally, we have known for years that punch size does not affect healing. Therefore, we have never allowed this punch size discussion to affect our procedure. Rather, we have continued to focus on one thing….RESULTS. This means we do not favor a single instrument exclusively. In fact, we are not immune to results that did not meet our expectations. Three years ago, we did not have all the options available to us that we have today. Increased variability and better quality instrumentation have allowed us to over come the challenging cases that we occasionally faced. The value of this technological progress has been consistent results.
More recently we decided to do a study and simply show objectively that there is no difference in healing regardless of what size punch you use. This is of course provided that you are able to get the hair out. If you are not able to get the hair out, the skin will heal just like it was prior to the procedure and both your donor and bald top of the scalp will look exactly the same or there will be little improvement because only a small number of viable hairs will be relocated to the bald or thinning areas.
In this study we compared our 0.75 mm punch with a punch significantly larger. The results of this study showed there was no statistically different appearance in the donor area. In fact the larger punch healed better.
What happens when you remove an intact follicular unit from the donor area? You eliminate a metabolically active structure from the surface of the skin. The structure requires blood flow to survive. It also produces color through the function of the melanocytes. Melanocytes produce melanin that can be seen in the hair and also as a colored shadow as the hair approaches the surface of the skin. Blood flow to the hair follicles is pink due to the presence of oxygenated hemoglobin in the red blood cells. Melanin produces a dark hue in the surrounding skin. When you remove the hair follicles, you reduce the pink color and the dark hue of the hair shafts. This can leave a lighter colored area of skin where the follicular group used to exist. This lighter color is equal regardless of whether you use a very tiny punch or a slightly larger punch.
There are a couple of ways to minimize this affect. One is to harvest only non-pigmented or grey hairs. Another is to harvest only a portion of a follicular group so that one or more hairs from the follicular group remain in the donor area. This scenario leaves metabolically active hair and pigment in the donor area so there is little or no color change. Another is to fractionate the follicular group through poor technique or the exclusive use of a punch that is too small for the donor area you are attempting to harvest. Still another is to place a body hair in the extraction site so that metabolically active hair and pigment are relocated to the donor area. Yet another is to harvest white hair that contains no pigment so the surrounding donor area appears the same.
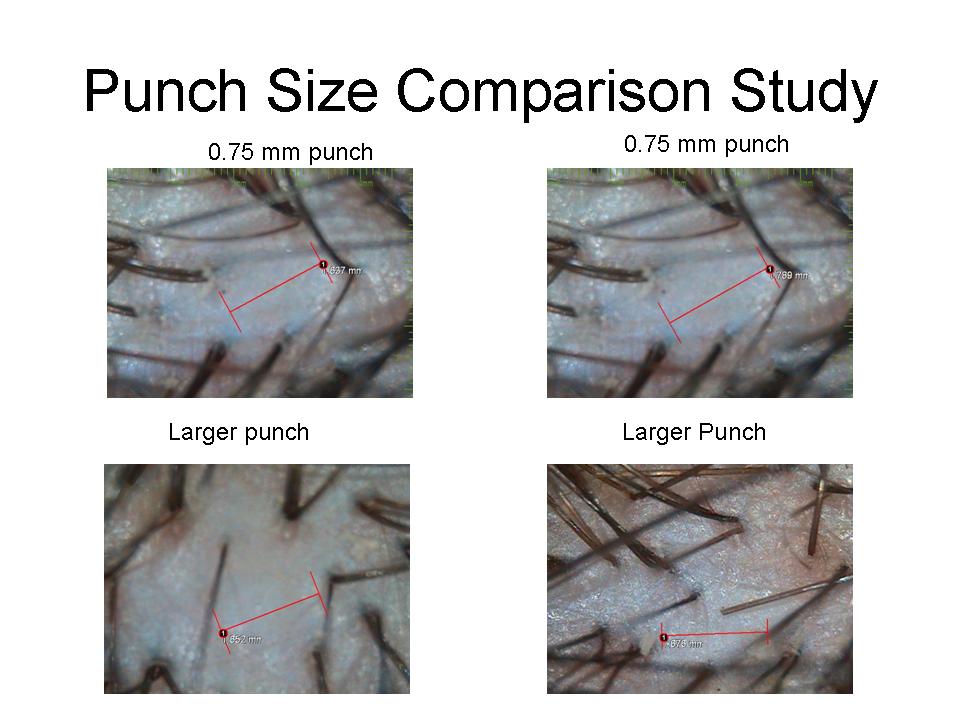
The region of less pigment at the extraction site is often called scar tissue by those who criticize FUE and those who promote strip surgery. These are not scars really. They are areas of less pigment due to less blood flow and less melanin than the surrounding areas. A successful extraction will leave a lighter area regardless of the size punch you use. This area of hypopigmentation is not evident in some with a bic cut and not evident in others cut to a number 1. This compares to what one sees with strip surgery where there is generally some scarring evident with changes in hair direction angles even with a trichophytic closure following a strip procedure. To illustrate this point note that the region of lighter color was measured in these photos comparing two different punch sizes. The examiner was blinded to the different size punch used in the two mirror image extraction regions on contralateral sides of the donor area. You will note that the hypopigmentation is larger than the punch used for both extraction sites and that the area of hypopigmentation is greater in the 0.75 mm punch extraction site. At 100X the change in color is minimal for both punch extraction sites, however. Scars do not spread and they do not expand in size unless you have keloid scarring, which is uncommon in a donor area to begin with and has never occurred in my hands when performing CIT™ . Keloids are raised scars. These areas of hypopigmentation are not raised. They are flat. Even strip scars do not expand beyond the size of the excision. You may see a 5 mm wide strip scar following a well performed strip procedure that is 1 cm wide, but you are not going to see a scar greater than 5 mm unless you perform some horrible technique that no quality surgeon is capable of performing. The hypopigmentation is present simply because the region requires less blood flow due to the removal of the follicular unit and they also no longer have hair follicles that produce pigment.
In summation, the hypothesis that a 0.75 mm punch produces less scarring in FUE is null. It was a good theory and this is why I introduced it in the first place way back in 2003. Unfortunately, the theory is worthless except as a marketing tool. The 0.75 mm punch has it’s place and we use a punch smaller than the 0.75 mm punch we introduced in 2003 when applicable. The internet debate over punch size continues to frighten some patients. Those individuals who are frightened often present to our office with a request that we use our smaller punches exclusively. I have no problem complying with this request provided that the patient is willing to sign a consent releasing our clinic from a higher probability of a poor result. It is very important to recognize that the punch size debate is one perpetuated predominantly by laymen. You see very few physicians bring the subject matter up. Patients should try to understand that laymen promote this smaller punch as a sales tool. Patients need to recognize that clinics who promote the smaller punch do not always use the smaller punch. Patients need to recognize that laymen are not in control of their surgical procedure or their surgical result. Patients should not trust the misguided and non-objective opinions or recommendations of laymen any more than they should trust a layman to perform their surgical procedure. Patients need to recognize that laymen promoting a smaller punch that has no objective data to support such an argument are doing so because they have a hidden agenda. In reality, it is false marketing and dishonesty at the highest level.
You have one donor area. That’s it. Once it’s gone, it’s gone. You have choices and you’ve had choices for many years. Many have made poor decisions and they are now repair cases or hair transplant victims. Today, many young men are allowing aggressive low hair lines and very high densities that often produce undesirable short and long term results. Others, are getting elevated follicular transection rates by physicians who do not understand how to properly perform FUE. At the recent ISHRS conference in Las Vegas, Nevada, transaction rates as high as 60% were noted by some physicians. That is 6 out of 10 hairs destroyed for the rest of your life and you will never get them back. I would not allow that physician to dictate my procedure any more than I would allow a layman who has even less of an idea how to perform FUE. Our transaction rate is about 3% on average. Sometimes it is under 0.5%.
Given that the hair transplant industry in general has produced over 50 years of poor aesthetic hair transplant results, I can understand that many patients want to believe that smaller is better in the case of FUE. No one understands this better than me because I spend approximately 50% of my time repairing patients who have run out of options in mainstream hair transplant surgery. Generally, by the time many of these repair cases get to my office, they have exhausted all other options and have limited donor resources despite a tremendous amount of hope. In order to overcome these obstacles, I have invented many procedures and instruments out of necessity. The work I do is equivalent to remolding a kitchen but having to re-use the same boards, drywall, and nails because no other supplies are available. Such work requires ingenuity and out of the box thinking. One instrument that I introduced to hair transplant surgery purely for aesthetic reasons was the 0.75 mm punch. Unfortunately, it is a tool that has limited applicability that carries far more risk than reward. It is also a tool that long term offers no aesthetic advantage to the donor area and far less growing hair in the recipient area.