HairSite EXCLUSIVE!
A new article on hair transplantation, published by Dr. Ray Woods, inventor and world pioneer of FUE (Follicular Unit Extraction) and BHT (Body Hair Transplant).
Baldness Donor Ratio (BDR)
1_file6.pdf
The Woods Ratio Baldness Donor Ratio (BDR)
A Remote Assessment Tool for Hair Transplant. The Baldness to Donor Ratio Method, The Woods Ratio: Dr Ray Woods MBBS,
Introduction
For clinicians engaged in hair transplant it is vital that there is clear communication with patients about realistic cosmetic outcomes [1]. Patient satisfaction is heavily reliant on meeting expectations; therefore clinicians should endeavour to ensure that both they and their patients are sharing a common understanding. The Baldness to Donor Ratio Method (BDR Method) is a tool to assist clinicians to communicate with patients about their possible cosmetic outcomes of hair transplantation.
With the rise of the internet consultation [2] and cosmetic tourism, potential patients want remote assessments to make their decisions and often invest considerable resources upfront for cosmetic services based on information given `sight unseen,. With regard to hair transplant, many clinicians rely on patient photographs and the Norwood Scale [4] that describes patterns of hair loss to make assessments. From research [5] and empirical observation it is evident that heads vary widely in shape and volume; therefore patterns of hair loss alone do not provide a satisfactory yardstick for clinicians to make accurate remote assessments.
In addition to the size of the bald area and limitations of available donor hair, other characteristics to be usefully considered in patient assessment for hair transplantation are the: contrast of hair colour compared to skin complexion; density of the donor site; pre-existing hair on the balding area and the diameter of the hair shaft. These characteristics taken together convey a clearer picture to inform a clinical opinion about achievable cosmetic outcomes and costs.
The internet is an influential communications tool and with the advent of blogs and chat forums it is also a powerful form of information and misinformation and a public record of patient satisfaction [3]. Clear descriptors will facilitate appropriate comparisons and discussion both between patients and clinician to patient. With the uptake of Follicular Unit Extraction techniques [6] the additional information about the patient characteristics allows a more accurate assessment as to the numbers of grafts, costs and expected cosmetic outcomes.
Aims and Objectives
The BDR Method has evolved over time in response to increasing demand for remote consultations and the observation that accurate assessments are not a simplistic function of baldness and donor areas.
The aim of the BDR Method is to provide a systematic way to collate descriptors affecting the cosmetic outcomes of hair transplant surgery. This will lead to:
*more accurate assessment by clinicians as to expected patient outcomes;
*easier evaluation and comparison of options for a second opinion;
*a systematic method for clinicians to record decisions in the patient record;
*a transparent and reproducible approach to patient assessment and costing;
*Assist patients to exchange information using common descriptors therefore reducing misinformation particularly on the internet forums and
*Increased patient satisfaction with hair transplant as patients will have realistic expectations as to their cosmetic outcomes.
Method
The BDR Method is a simple two part process incorporating patient characteristics that in addition to baldness should be considered in assessing a patient for hair transplantation.
Patients complete a semi -quantitative self assessment to give a ratio of their 'bald to donor, areas plus a qualitative self assessment. The process described below.
Part 1. A semi quantitative assessment:
Ratio of bald area to donor area: A useful measurement technique is to take a thin cloth, or paper and trace around the bald and donor areas; A visual approximation will suffice to assign a ratio. For example a ratio of 1:1 = Ration = 1 indicates the patient has 50% of the scalp covered with hair and 50 % balding. 2:1 = Ratio = 2 indicates the bald area is twice a big as the donor area. Therefore the higher the Ratio the less donor head hair. This method is simple, robust and accounts well for variations in skull volume and shape.
Part 2. A qualitative assessment. The patient selects their skin and hair characteristics from the options below.
*Donor density (DD): Thin, Medium, Thick — The thicker the donor hair the more available for grafts.
*Diameter of the donor hair shaft (SD) : Fine Medium Coarse; The coarser the hair shaft the greater the coverage
*Colour Contrast (CC): Low, Medium, High - colour contrast between hair and complexion. For example black hair and white skin is high contrast while grey hair and white skin is low contrast
*Pre existing hair (PE): Zero, Sparse, Medium — This describes the current hair coverage in the balding area
Results
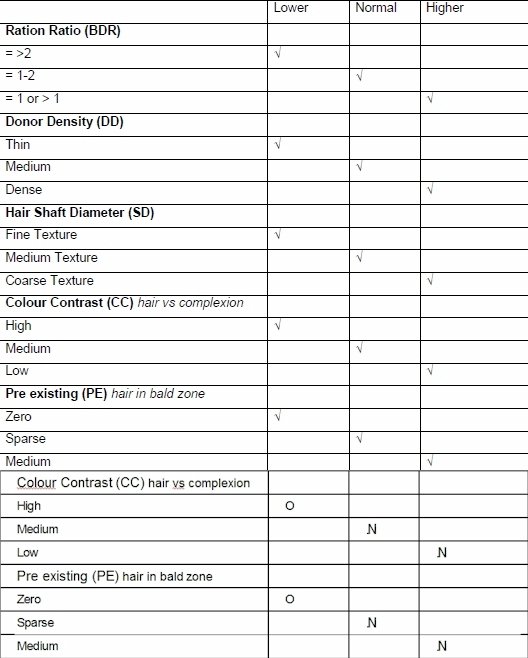
Table 1 Summary of the BDR Method: Characteristics and their effect on hair transplant coverage.
Discussion
By systematically summarising their information across five parameters patients can clearly communicate their case details to a clinician. From Table 1. an appraisal can be easily made for characteristics that will affect the a patient,s possible cosmetic outcome. For example patients with a ratio of bald to donor 1:1, dense donor area, coarse hair, low colour contrast and medium pre-existing hair would be summarised as:
Ratio =1 / DD Dense / SD Coarse / CC Low / PE Medium.
In this example the patient has very favourable characteristics that would support expectations for a good cosmetic result. To note, additional donor hair may be available from chest hair if the patient is suitable [7].
Conclusion
Patient demand for internet consultations challenges clinicians to accurately assess and manage outcome expectations for hair transplantation. In addition to the bald area and limitations of the donor site: Patient characteristics such as contrast between the hair colour and skin complexion; the density of the donor site; the pre-existing hair on the balding area and the diameter of the hair shaft are important factors. Patient self assessment using the Baldness to Donor Ratio (BDR) Method can provide semi-quantitative and qualitative data to assist clinicians in remote assessments. The BDR Method is a tool: To increase the accuracy of clinicians making remote assessments; to provide clinicians with a systematic approach to documenting the patient record; increase transparency as to how assessments and costs are derived and assist patients to evaluate second opinions. In addition to the above, given the extraordinary use of consumer internet forums in the field of hair transplant, the BDR Method can facilitate discussion with agreed descriptors thereby supporting patients in forming realistic expectations. Given the link between expectations and cosmetic outcomes, it is anticipated that patients holding realistic expectations will have higher levels of satisfaction.
============
1 Rohrich, R J. Mirror, mirror on the wall: when the postoperative reflection does not meet patients’ expectations. Plastic & Reconstructive Surgery. 108(2):507-9, 2001 Aug.
2 UmefJord, Goran. Sandstrom, Herbert. Malker, Hans. Petersson, Goran. Medical text-based consultations on the Internet: a 4-year study. International Journal of Medical Informatics. 77(2):114-21, 2008 Feb
4 Norwood OT: Male Pattern Baldness: Classification and Incidence. South M J 1975, 68:1359-1365
5 Ahmet Rifat Ormecci, Huseyin Garbaz, Ali Ayata, Hasan Cetin Adult Head Circumferences and Centiles Journal of Turgut Ozal Medical Centre (4) 3: 1997
6 Gokrem S. Baser NT. Aslan G. Follicular unit extraction in hair transplantation: personal experience. [Journal Article] Annals of Plastic Surgery. 60(2):127-33, 2008 Feb
7 Woods R. Campbell AW. Chest hair micrografts display extended growth in scalp tissue: a case report. [Case Reports. Journal Article] British Journal of Plastic Surgery. 57(8):789-91, 2004 Dec
Dr. Woods is the inventor of FUE and BHT technique and is a sponsoring physician of HairSite. For patient results or more information about his work, please go to www.woodstechnique.com.au
The videos and photos you see on HairSite are provided by our paid sponsors and are not endorsed by HairSite in any way. HairSite does not warrant the information provided in any of the videos or photos featured on this site. The recommendations, results, and representations made by our sponsors do not reflect the opinions, experiences, findings, or experiences of HairSite.



