» Quote
» Any physician can confirm the previous statements. We turn down over one
» hundred patients who wish to do surgery but we don’t suggest for surgery.
» We get numerous patients in their early 20s who didn’t know that they even
» had a linear scar. Don’t tell me that it “sounds” like at sales pitch when
» the statements are factual
»
» CIT,
» You said that any physician can confirm your previous statements. If that
» is so, I believe is it important,no i think it is essential that a
» physician, any physician not associated with your clinic corroborates your
» story. In particular i would greatly appreciate hearing about your
» “introduction” of the .75mm punch from an objective third-party. The reason
» for my interest in this matter is that I have yet to hear any doctor in
» person or online ever state that you introduced the .75 or any punch for
» that matter. What is more i believe that many doctors have expressed
» concerns that you use a large punch technology (that is punches greater
» than 1mm in diameter). So again i humbly request that a doctor (outside of
» your group) support your story. FUE doctors who post on this site include:
» Dr Woods the inventor of FUE, Dr Umar the chief surgeon of an all only FUE
» clinic in the US (no strip), Dr Jones the first doctor to offer FUE
» surgery in the North America, Dr Bisanga a surgeon who has produced some
» of the finest .75mm FUE results to ever grace this website, Dr Poswal, Dr.
» Feller, and numerous others.
»
» Your responses in this thread have been clever but in my opinion salesy.
» You appear to be avoiding very concrete and easy to answer questions. This
» sort of behavior, as I am sure you can understand might lead the public to
» believe that you are hiding something.
Good Evening Bigmac,
As I have said it once, I shall say it again. Our clinic doesn’t market our service as the majority of clinics do. What seperates our procedure from the rest is the simple fact that it provides the most consistent quality results in the industry. They remain consistent and undetectable while adding more coverage with fewer grafts.
If you do some research on FUE, you will find that FUE clinics don’t quite produce the quantity or quality that CIT procedure produce. Furthermore,
CIT incorperates instrumentation that is tailored to each specific patient’s needs with a full-time engineer on-staff. You will also note that the discussion of the smaller instruments introduced by Dr. Cole have yet to be contested by only zero physicians on this hair loss forum.
Your initial statement was "I would like to see these inferior results from other top clinics you have repaired/refined as i will be able to search and find unhappy patient results from you as well. " I charge you with finding CIT cases in need of repair. Many, if not all of these repair patients want help to organize the madness that they have endured.
My fellow forum viewer,
All you can do is research online facts in regard to CIT and critique the results that have been produced. You may or may not be truley interested in the positive outcome of these cases (video & photos) and perhaps you may or may not have your own agenda.
Your question in regard to the introduction of the aformentioned smaller instrument may be researched by youself or other inqiring minds on the front page of our website. Here’s the link for your convenience: forhair . com / Articles / Punch_Size_Comparison_Study_in_Hair_Transplant_Surgery . htm
Our approach is “more is less” as we encourage our patients to consider any future loss. There is no marketing but there is factual information. Like, Dr. Cole has practiced FUE/BHT longer that any other surgeon in the U.S.A. Your invitation to other doctors of the forum is greatly appreciated.
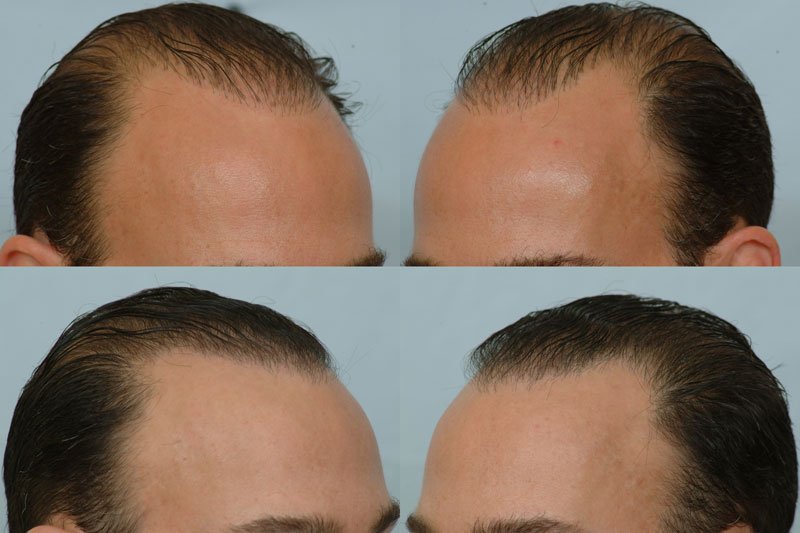
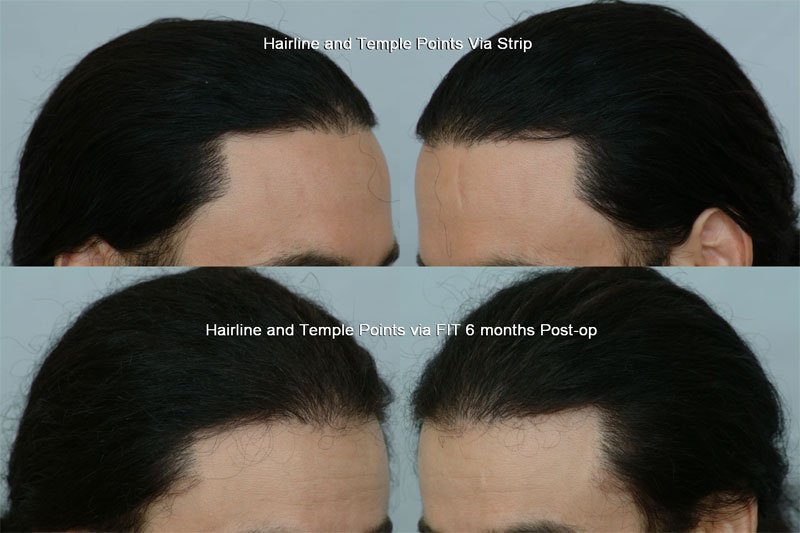
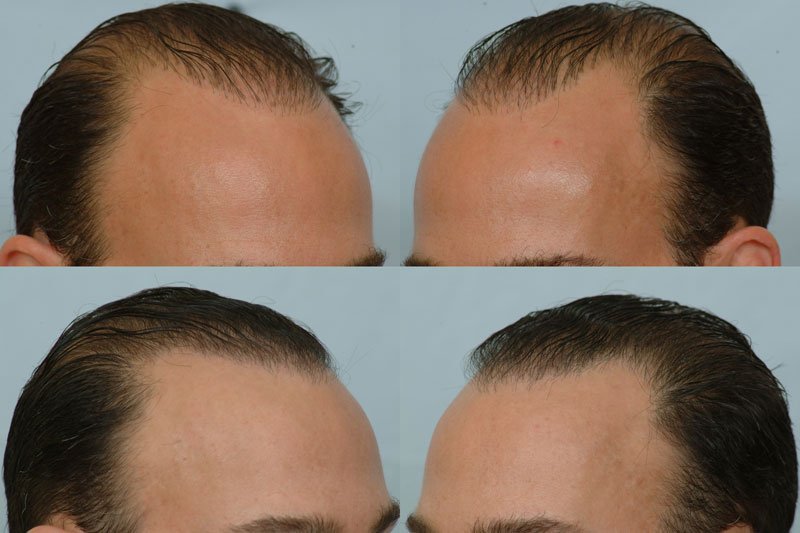
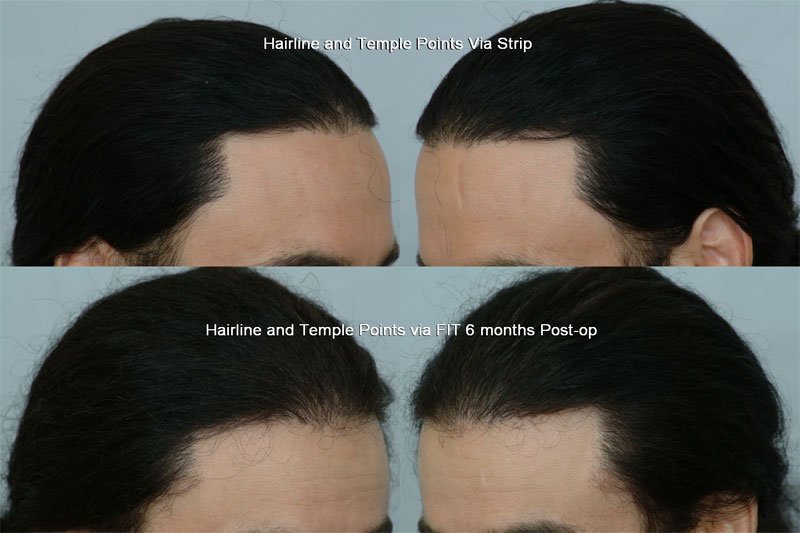
Regarding the following statement, "I would sincerely appreciate it if you could substantiate your claims that your procedure, CIT, is superior to all other FUE procedures. I could understand it if you felt your surgery was good, or something like that. But I would like to know why it is superior to all other FUE procedures. I would also like to know how you know this, particularly since you are not monitoring surgeries at other clinics. Finally, I would like to know whether or not you believe that your statements are really objective. Yes, they are objective and here’s the evidence:
Entire database of hair transplant patient stats - There is nothing else more to say
_file4.wmv
My advice is not medical advice