Dr. Bisanga has adapted and improved his FUE punch technique over the years, one obvious example is the size of punch he uses has dropped in diameter to minimise traumatic impact on the scalp and surrounding follicular units. Another aspect is the technical ability and objective technique, the ability to feel the follicular unit and surrounding tissue when entering the scalp and gauging the depth and angles of each FU.
During my FUE sessions I was always aware of the changing positions Dr. Bisanga used to make, moving himself and adapting to changes in the angles and directions of the FU. Now watching FUE punching from the other side I have seen more.
FUE has and will always be technically a very difficult technique, the fact that each FU has to be removed individually and the average op is 1000 grafts plus obviously multiplies the room for error as each extraction can be different in some cases. Dependent on the area of the scalp,the angle the FU exits the scalp changes, dependent on the area it can be easier to extract the FU as the lay of the FU can be more consistent and also the position of the head when resting on the operating chair allows for easier extraction.
For example the back of the head, around the occipital area is much easier to punch. It is important the doc can understand his position needs to change otherwise there will be a greater scarring impact and potentially increased transection. The constant need to change position is not something that can be avoided regardless of tool size or the type of tool, this is about the technique itself.
Pressure control is also important to achieving minimum transaction and the least potential trauma to the surrounding FU. A largely forgotten aspect to FUE is the effects on the surrounding FU that are left in the donor. A FUE donor maybe be spread over the entire donor safe zone and if used well can leave minimal to almost no signs hair has been removed, but incorrect punch and extraction can greatly reduce the potential for future FUE and the graft numbers and even hinder Strip extraction.
The greater the friction created when the punch enters the skin the harder to balance the direction of the hair with any potential changes as there becomes less sensitivity between the fingers and the tip of the punch. The tension can be micro but Dr. Bisanga has found through changing his technique that even manually the tension can be reduced and this improves graft survival and collateral damage. The finger to punch pressure helps gauge the skin characteristics and even possible to feel the FU with practice. With this technique of punching Dr. Bisanga has minimised transaction to as little as 1-2% in most cases and even on demanding cases rarely increases to above 5%; this is only made possible by the touch sense gained through minimal transference of distance and resistance between his fingers and the punch.
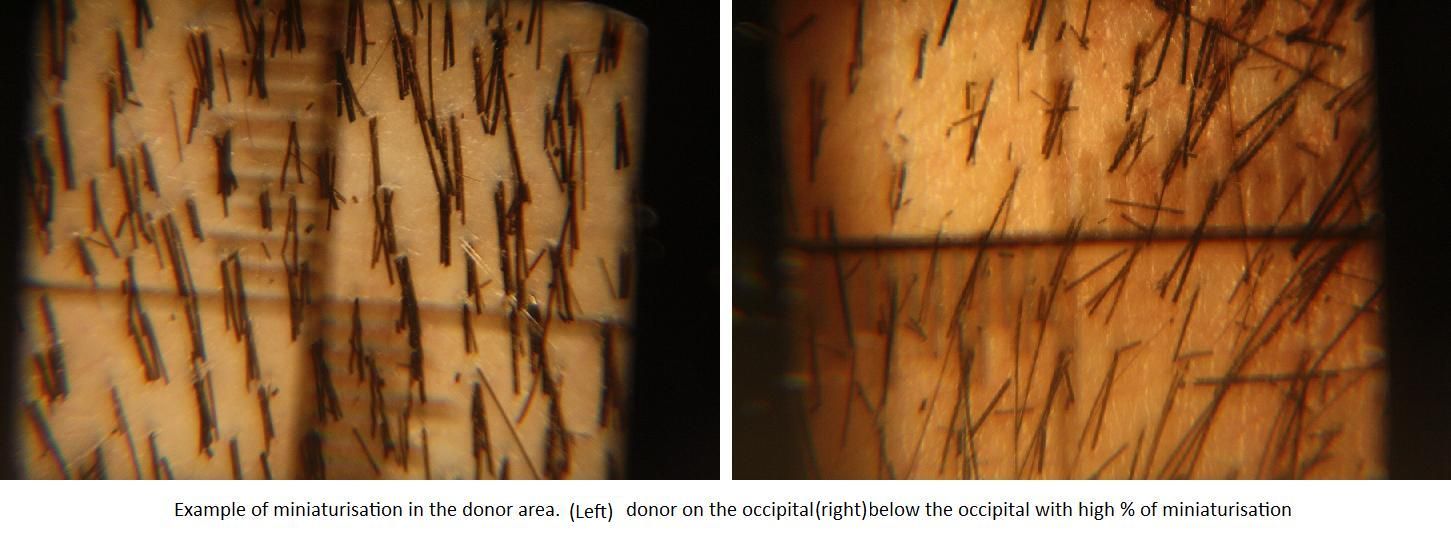
The next aspect that is over looked much of the time is miniaturisation existing in the donor and the potential to create miniaturisation. Dr. Bisanga feels that anything near 20% miniaturisation in the donor can rule you out from surgery, certainly having FUE. Miniaturisation does not affect the density of the donor hair as such because that is just the calculation of FU per cm2 but it will affect the number of FU that can be removed. We have seen miniaturisation spread all over the donor and also just in isolated areas, either way it will reduce the numbers that can be extracted. By definition the miniaturised hair cannot be used so they must remain in the donor, this creates the problem of how close to the miniaturised FU can the extraction take place. Too close and the thickness of coverage will drop and could potentially traumatise the miniaturised hair and cause it to fall out.
So, the extraction pattern has to become wider thus less FU per cm2 are removed to retain the integrity of the donor, especially for the future. Miniaturisation can also be caused with the extraction, going back to the tension or resistance in the punch movement, this can create a ripple effect, like a “skin quake”, the punch hole being the epicentre and the vibrations moving out from the central point. As above Dr. Bisanga has minimised aspects of this by his punch motion technique, he has certainly found less resistance was caused creating obviously less contortion of the wound and the surrounding Follicular Units. This is very important, we have seen miniaturisation created post FUE surgery that has possibly rendered the areas non- harvestable due sometimes to over harvesting but also peripheral damage creating miniaturisation.
Dr. Bisanga’s feeling on these problems is to lessen the motion when making the punch action, the least friction or motion allows for greater sensitivity and feel between punch and fingers and this in turn has reduced transection, decreased peripheral damage either to the skin or surrounding FU with changing directions as well as miniaturisation. With the many documented FUE cases he has to his name as well as the many more he has performed and internally documented he feels confident to say that in respect of physical technique he has reduced these negative factors a great deal but then research is obviously ongoing.